60 Flu Vaccinated People Die Of Flu, And 33 Unvaccinated People
Influenza has killed 93 children under age 18 since last October, but there is no way to determine whether the current season is more severe for children than earlier years, the Centers for Disease Control and Prevention said today.
The vast majority, 33, or 73 percent, had not been vaccinated. The C.D.C. recommends that all healthy children 6 months and older be vaccinated.
Source: The New York Times, January 8th 2004.
VAN UK’S Comment: I’d like to know how they work out that the majority were unvaccinated when 93 children died, and of those 33 were unvaccinated. That means that 60 were vaccinated!
Flu Vaccine Has No Effect For Children With Cancer
Community acquired influenza can be severe and there are few data regarding hospitalization for children with cancer and influenza. Association between prior vaccination and infection severity has not been studied, although vaccination is standard practice.
Procedure
Patients with malignancy or prior stem cell transplant (SCT) were identified using a database of children with laboratory confirmed influenza (2000-2005). Other data collected included receipt of vaccine, absolute neutrophil count (ANC) and absolute lymphocyte count (ALC). These were compared with intensive care unit (ICU) stay, respiratory complications and hospital days.
Results
There were 39 patients with laboratory-confirmed influenza with a median age of 6.9 years. Twenty-four (62%) were on cancer therapy at time of infection and 18 (46%) had received the influenza vaccination that season. Measures of immune status included ANC at time of infection (median 1,530 cells/µl; inter-quartile range, 315, 4347), presence of graft versus host disease 2 (5%) and steroid therapy 4 (10%) patients. All had a low ALC (median 448 cells/µl; IQR 189, 861). Respiratory complications occurred in 8 (20%), ICU admissions in 4 (10%) and death in 2 (5%) patients. Median hospital stay was 2 days. All ICU admissions occurred in unvaccinated patients (P = 0.1). Vaccine status, ANC (<1,000 cells/µl vs. >1,000) and ALC (<500 cells/µl vs. >500) were not associated with length of stay or respiratory complications.
Conclusions
Influenza infection can be severe in children with cancer and complications occur despite vaccination. Prospective evaluation of vaccine response is worthy of future study. Pediatr Blood Cancer © 2009 Wiley-Liss, Inc.
Source: Pediatric and Blood Cancer,
.1002/pbc.22228.
Vaccinated Nurse Dies of ‘Swine Flu’
According to reports, a nurse and father of two, Kevin Hall, 43-years-old, passed away in arms of his wife Jennifer on Christmas Day, just two months after having the swine flu vaccination, as he was later confirmed to be killed by the H1N1 virus.
Also, a new breath test is being investigated to assist in identifying people infected with the H1N1 flu virus, and the test, which measures the immune response to the H1N1 flu virus, can assist in curbing future vaccine shortages by identifying people who have been infected with the flu virus and preventing irrelevant vaccinations.
However, the researchers, from Cleveland Clinic and Syft Technologies investigated the ‘fast-acting, non-invasive’ breath test to rate biomolecules that are brought together responding to the H1N1 strain. Hence, the breath test analyzed the exhaled nitric oxide a biomolecule, that its previous production has been connected to influenza, viral infection and presumed to have a favorable role in the elimination of the viral infection.
Moreover, the results revealed a rise in nitric oxide levels in all subjects on the third day after vaccination and there were no major differences in the levels on any of the other days.
Source: http://newstonight.net/content/nurse-dies-swine-flu-despite-vaccination
Deadly Flu Outbreak in Vaccinated People Shuts Centre for Disabled
Two Hunter region facilities for the disabled are in lock-down after a flu-outbreak and the deaths of three residents who had suffered flu-like symptoms.
In the past week, two men in their 60s and a woman aged in her 40s died at the Stockton and Kanangra Centres.
51 residents are now being treated for the flu and strict infection control measures have been introduced at the centres which house 450 people.
The Opposition Health spokesman, Doctor Andrew McDonald says he is concerned that it may be a new strain of flu.
“This is a great concern because most of these people had been vaccinated against the flu,” he said.
“This means that the vaccination is either ineffective or it’s a new virus.
“If there’s 450 people at these centres, it’s highly likely this virus will spread to other facilities in the area and elderly people will be at risk from this virus.”
Doctor McDonald says it is very concerning development this late in the flu season.
“This is a great worry because we know that July is the busiest month for influenza, so if we’re just having an epidemic now, there is always potential for it to get bigger,” he said.
“The great worry about these infections is that the vaccination is ineffective, it will come down to very careful infection control measures.”
Disability Services Minister Andrew Constance says strict control practices are now in place.
“Some residents are contained to their units in which they reside,” he said.
“We’re ensuring that cleanlieness and hygiene procedures at both centres have been intensified and staff at both centres are wearing protective equipment.”
Source: ABC News, 3rd August 2012 – http://www.abc.net.au/news/2012-08-03/deadly-flu-outbreak-shuts-centres-for-disabled/4174152
VAN UK’S COMMENT: They didn’t consider the possibility that the vaccines caused the flu outbreak, rather than simply being ineffective.
Outbreaks in Vaccinated Staff
Researchers from the British Columbia Centre for Disease Control observed suboptimal vaccine effectiveness against the influenza A/H3N2 virus during the 2010-2011 winter season and also detected genetic variants to the virus using a sentinel surveillance platform.
During this time frame, there were many outbreaks related to influenza A/H3N2 at long-term care facilities in Canada. The outbreaks also affected vaccinated staff. Interim data from the sentinel surveillance system, which incorporated genotypic, phenotypic and epidemiologic indicators, identified genetic variants and suboptimal vaccine effectiveness.
“Unlike other vaccines, the influenza vaccine must be reformulated and re-administered each year to keep pace with ongoing changes in circulating virus strains,” Danuta Skowronski, MD, epidemiology lead of Influenza & Emerging Respiratory Pathogens at BC Centre for Disease Control, told Infectious Disease News. “For this reason, real-time monitoring of circulating strains, their relatedness to chosen vaccine components and their impact on vaccine protection are important. To do this requires the efficient harnessing of molecular, individual and population-level information.”
The researchers analyzed nasal/nasopharyngeal swabs and epidemiologic data from 1,718 participants who presented with influenza-like illness. Among these participants, 93 tested positive with A(H1N1)pdm09, 408 had A/H3N2 and 199 had influenza B. Patients who tested negative for influenza were considered controls. Among the cases, 16% received the influenza vaccine and among the controls, 24% received the vaccine.
The vaccine efficacy for adults aged 20 to 49 years was 65% for A(H1N1)pdm09 and 66% for influenza B. For A/H3N2, however, the vaccine efficacy was only 39%.
Two hundred thirty-three specimens were isolated for hemagglutination inhibition characterization. This process showed that all of the A(H1N1)pdm09 isolates were A/California/7/2009-like and all of the A/H3N2 isolates were A/Perth/16/2009-like, demonstrating that all of the isolates were well matched to the vaccine. However, on phylogenetic analysis, only two of the A/H3N2 isolates belonged to the A/Perth/16/2009 vaccine clade. Most belonged to the A/HongKong/2121/2010 variant, and the remainder belonged to the A/Victoria/208/2009 variant, both of which were not matched to the vaccine.
Source: Infectious Disease News, 3rd August 2012 – http://www.healio.com/infectious-disease/vaccine-preventable-diseases/news/online/%7B90A188FA-50CB-4206-A557-FFE927905EDE%7D/Suboptimal-vaccine-effectiveness-against-influenza-AH3N2-identified
Influenza Outbreak in a Vaccinated Population — USS Ardent, February 2014
Theodore L. Aquino, DO1, Gary T. Brice, PhD2, Sherry Hayes, MPH3, Christopher A. Myers, PhD2, Jaqueline McDowell, MD3, Brenda White, MSPH, MPH2, Rebecca Garten, PhD4, Daniel Johnston5 (Author affiliations at end of text)
On February 10, 2014, the USS Ardent, a U.S. Navy minesweeper, was moored in San Diego, California, while conducting training. Over the course of 3 days, 25 of 102 crew members sought medical care because of influenza-like illness (ILI). Nasal swab specimens were collected from each patient, and initial rapid influenza testing indicated 16 cases of influenza A. Ultimately, polymerase chain reaction (PCR) testing conducted by the Naval Health Research Center determined that 20 specimens were influenza A, of which 18 were subtype H3N2. Two specimens could not be subtyped. The HA gene sequence of an outbreak isolate was 99% identical to strains circulating during the 2013–14 influenza season and antigenically similar to the H3N2 component of the 2013–14 influenza vaccine. At the time of the outbreak, 99% of the crew had received influenza vaccine. Through the duration of the outbreak, the minesweeper squadron medical officer collaborated with Navy Environmental and Preventive Medicine Unit Five, higher-level Navy authorities, and County of San Diego Public Health Services to implement the outbreak response, which included disseminating outbreak information to surrounding Navy units, disinfecting the ship, sending home infected crew members, identifying family members at high risk, and providing antiviral medications and guidance. No crew member had onset of symptoms >6 days after the first crew member became ill. This outbreak highlights the risk for an H3N2 influenza outbreak among vaccinated and otherwise healthy young persons.
ILI was defined as illness with two or more of the following symptoms: fever >100.4°F (>38.0°C), chills, sore throat, cough, shortness of breath, congestion, headache, body aches, and nausea. Twenty crew members reported sick on February 10, one on February 11 and four more on February 12. Symptom onset dates were February 5–11 (Figure). All ILI patients were interviewed and examined aboard ship by both an independent duty corpsman (i.e., shipboard medical provider) and a physician. Two nasal swab specimens were taken from each ILI patient by staff members from the Naval Health Research Center. Nasal swab specimens and influenza A and B rapid influenza tests were used for immediate influenza testing. The remaining nasal swab specimens were screened by the Naval Health Research Center for influenza A and B using the CDC PCR assay (1), and DNA sequencing of the HA1 portion of the hemagglutinin gene was performed as previously described (2). Data on demographics and symptomatology were collected using questionnaires and personal interviews.
All 25 crew members with ILI symptoms were otherwise healthy men aged 21–44 years. ILI cases occurred in all ranks, departments, job types, and work shifts. The ship had been in port since being transported from Bahrain to San Diego 2 months before the outbreak. No sailors reported any recent travel. Rapid influenza testing indicated 16 cases of influenza A and nine negative results. Nasal swab specimens from 20 of the 25 ILI patients were positive by PCR for influenza A, with 18 specimens confirmed as A (H3) and two as A (untyped). Influenza A virus was isolated from seven of 11 nasal swab specimens selected for viral culture. These seven specimens had HA1 protein sequences that were identical to each other and differed from the 2013–14 influenza A (H3N2) A/Texas/50/2012 vaccine strain by 5 amino acid substitutions (N128A, R142G, N145S, P198S, and V347K). Sequence analysis (3) of the HA1 portion of the hemagglutinin gene showed 99% homology to typical H3N2 strains circulating in the United States and worldwide during the 2013–14 northern hemisphere influenza season and were found to be antigenically similar to A/Texas/50/2012 (4). Ninety-nine of 102 USS Ardent crew members, 24 of the 25 with ILI symptoms, and 17 of 18 crew members with confirmed influenza A (H3N2) infection had received the 2013–14 influenza vaccine ≥3 months before the outbreak. Vaccinations had been administered at local naval health clinics and at a vaccination fair conducted by Naval Medical Center San Diego. Of the 25 crew members with ILI symptoms, 16 were vaccinated via intradermal injection, eight via intranasal mist, and one had not received vaccination.
Interviews revealed a possible source of the outbreak to be an Ardent crew member (patient A), aged 26 years, who had been evaluated at a local emergency room for fever and cough on January 30, 11 days before the first ILI case was diagnosed. A chest radiograph and computed tomographic scan were performed because of suspicion of pulmonary embolism; both were negative. The patient had been receiving treatment for pyelonephritis, and the clinical impression was that the cough was related to the pyelonephritis. No testing for influenza was performed, and the patient was discharged. Patient A’s roommate in a shore apartment, also a USS Ardent sailor, experienced ILI symptoms on February 5. Because patient A’s roommate was the first of the 25 crew members to experience ILI, and no other probable cause for the outbreak was found, it is possible that patient A actually had influenza. Since patient A did not board USS Ardent because he was ill, it is likely he infected his roommate, who then spread influenza to other USS Ardent crew members.
In an effort to reduce spread and impact of disease, oseltamivir (75 mg twice a day for 5 days) was prescribed to each ILI patient who reported that symptoms had developed within 48 hours of their medical visit, regardless of their vaccination status and rapid influenza testing results. In addition to antiviral medication, rapid identification of the influenza outbreak, and immediate isolation of affected persons (crew members with ILI symptoms were sent off ship to their homes for 48 hours), additional steps to control the outbreak were taken: thorough cleaning of spaces throughout the ship by the crew and use of the ship’s public address system to instruct personnel to wash hands frequently, use hand sanitizer, cover their mouths when coughing, and report for medical evaluation if they were experiencing ILI symptoms. Similar announcements were made aboard three other minesweepers sharing the same pier as USS Ardent. Following a policy implemented by the independent duty corpsman, all patients experiencing ILI symptoms were required to wear an N95 filtering facepiece respirator while shipboard until 5 days after onset of symptoms. Cleaning of spaces was done by regularly disinfecting all commonly touched surfaces with disinfecting wipes and mopping all decks with an iodophor disinfectant diluted to 150 ppm of iodine. E-mails and reports regarding the outbreak, with an emphasis on rapidly identifying patients with ILI, were distributed to all ships on Naval Base San Diego and to high-level Navy officials and County of San Diego Public Health Services. No additional cases were identified after February 14. A total of 43 working days were lost by the 25 ILI patients.
Discussion
USS Ardent, an Avenger class minesweeper, is one of the smallest ships in the U.S. Navy. It has one shared space in which the entire crew eats meals. Work areas are spread throughout the ship, and there are nine sleeping spaces. Military populations, especially those living and working in confined settings, are susceptible to respiratory disease outbreaks (5). Shipboard personnel are at especially high risk because of constant close quarter exposure to a large number of crew members (6). Virtually all areas onboard ships are shared, and movement frequently requires touching handrails, door knobs, and other objects that can be contaminated with nasal secretions. In addition, ventilation systems can circulate infectious pathogens throughout a ship (7).
As the ship was moored in San Diego, the entire crew worked onboard during the day, and 25% remained onboard through each night. The roster of crew members who remained onboard at night rotated daily. There were 16 cases of confirmed influenza A (H3N2 )infection in San Diego County (Brit H. Colanter, MPH, Health and Human Services Agency County of San Diego, personal communication, 2014) during the 6 weeks leading to the ship outbreak, making it likely that the virus was acquired from the local community.
Since the 1950s, a policy of mandatory annual vaccination against influenza for active duty personnel has been largely successful in limiting influenza epidemics in the military (8). The current U.S. Department of Defense influenza vaccination policy mandates that all uniformed personnel receive seasonal influenza vaccination, unless medically exempt, or face punishment under the Uniform Code of Military Justice. The policy specifically directs all Navy operational units to be at least 90% vaccinated. However, despite vaccination measures, influenza outbreaks can still occur in highly vaccinated military populations (9,10).
References
- Shu B, Wu K-H, Emery S, et al. Design and performance of the CDC real-time reverse transcriptase PCR swine flu panel for detection of 2009 A (H1N1) pandemic influenza virus. J Clin Microbiol 2011;49:2614–9.
- Faix DJ, Hawksworth AW, Myers CA, et al. Decreased serological response in vaccinated military recruits during 2011 correspond to genetic drift in concurrent circulating pandemic A/H1N1 viruses. PLoS One 2012;7:e34581.
- Altschul SF, Madden TL, Schäffer AA, et al. Gapped BLAST and PSI-BLAST: a new generation of protein database search programs. Nucleic Acids Res 1997;25:3389–402.
- World Health Organization. Recommended composition of influenza virus vaccines for use in the 2013–2014 northern hemisphere influenza season. Wkly Epidemiol Rec 2013;88:101–16.
- Vera DM, Hora RA, Murillo A, et al. Assessing the impact of public health interventions on the transmission of pandemic H1N1 influenza a virus aboard a Peruvian navy ship. Influenza Other Respir Viruses 2014;8:353–9.
- Kak V. Infections in confined spaces: cruise ships, military barracks, and college dormitories. Infect Dis Clin North Am 2007;21:773–84, ix–x.
- Li Y, Leung GM, Tang JW, et al. Role of ventilation in airborne transmission of infectious agents in the built environment—a multidisciplinary systematic review. Indoor Air 2007;17:2–18.
- Gray GC, Callahan JD, Hawksworth AW, Fisher CA, Gaydos JC. Respiratory diseases among U.S. military personnel: countering emerging threats. Emerg Infect Dis 1999;5:379–85.
- Earhart KE, Beadle C, Miller LK, et al. Outbreak of influenza in highly vaccinated crew of U.S. Navy ship. Emerg Infect Dis 2001;7:463–5.
- Cosby MT, Pimental G, Nevin RL, et al. Outbreak of H3N2 Influenza at a US Military Base in Djibouti during the H1N1 pandemic of 2009. PLoS One 2013;7:e82089.
What is already known on this topic?
The single best way to prevent influenza infection is to receive vaccination every year. Some organizations have a mandatory vaccination policy. Despite this, influenza outbreaks can occur in highly vaccinated populations, especially in confined settings.
What is added by this report?
In February 2014, a total of 25 of the 102 crew members of a U.S. Navy minesweeper sought medical care because of influenza-like illness attributed to an influenza A (H3N2) virus antigenically similar to the H3N2 component of the 2013–14 vaccine. Among the crew members, 99% had received influenza vaccination, including 24 of 25 ill persons. Outbreak management included use of an antiviral medication, exclusion of the ill from the ship for 48 hours, disinfection, hand washing, and cough etiquette. No crew member had onset of symptoms >6 days after the first crew member had symptoms.
What are the implications for public health practice?
This influenza outbreak highlights the risk for an outbreak of influenza A (H3N2) in a cohort of vaccinated and otherwise healthy young persons.
FIGURE. Number of cases (N = 25) of influenza-like illness, by date of symptom onset — USS Ardent, February 5–11, 2014
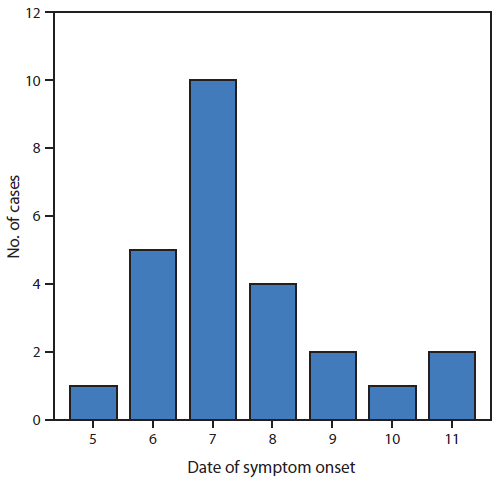 Alternate Text: The figure above is a bar chart showing the number of cases (N = 25) of influenza-like illness, by date of symptom onset on the USS Ardent during February 5–11, 2014. Twenty crew members reported sick on February 10, one on February 11, and four more on February 12. Symptom onset dates were February 5–11. Alternate Text: The figure above is a bar chart showing the number of cases (N = 25) of influenza-like illness, by date of symptom onset on the USS Ardent during February 5–11, 2014. Twenty crew members reported sick on February 10, one on February 11, and four more on February 12. Symptom onset dates were February 5–11.
Source: MMWR, October 24, 2014 / 63(42);947-949.
CDC report of outbreak on vaccinated navy ship
Girl, five, dies from a strain of the flu she was vaccinated against as deadly epidemic continues to sweep across the US
A five-year-old girl has died in hospital three days after developing a strain of the flu that she was vaccinated against – as a deadly outbreak of the virus continues to sweep across the country.
Keira Driscoll was prescribed steroids and a nebulizer at a Quick Care clinic after she started feeling unwell with a cough and a fever at her home in Clark County, Las Vegas, last Sunday.
But just hours later, she collapsed. Her mother, Tiffany Driscoll, frantically performed CPR on her small body, before she was rushed to hospital. There, she was found to have influenza A.
Despite medics’ best efforts, Keira could not be resuscitated and she was placed on life support. On Tuesday, her parents made the heartbreaking decision to turn off the machine the next day.
However, Keira died before the machine would have been switched off after suffering from a cardiac arrest. She was surrounded by her mother, father, Peter Driscoll, and other relatives at the time.
The youngster is the fourth child in the Nevada-based county – and the 56th nationwide – to have died from the flu in the past few months as vaccines have proved largely ineffective.
8 Year Old Vaccinated Girl Dies of Flu
8 Year Old Mackenzie Coyne of Park City died Sunday shortly after testing positive for influenza A. Her family said it progressed quickly over the weekend, even though she had a flu shot. Now the community is coming together for her family to help.
She celebrated her birthday last Friday when she told her dad she was a little under the weather. On Saturday her family urged her to rest and she did get sick once. They assumed she was sick like most kids get. By Sunday they noticed something was wrong and took her to the urgent care where she tested positive for influenza A.
Family friend Carrie Prater said that an ambulance rushed her to the hospital 20 minutes later, but things deteriorated fast. Shortly after arriving she was gone even though doctors tried to revive her.
“Literally went from bad to worse to she was gone.” said Prater. “It’s very unreal at this point.”
Utah Department of Health said there are tests they still need to run before they will confirm if the flu was directly related to her death. Her family was told by doctors that she could have had a secondary infection that caused her major problems, but the flu could have weakened her immune system.
Source: Good 4 Utah, 17 February 2016.
8 Year Old Vaccinated Girl Dies of Flu.
VAN UK’S Comment: We wonder when the vaccination was done as there is a latent phase between injections and side-effects developing in some cases and it may be that the vaccine caused the flu, rather than just failing to protect her.
26 Year Old Newlywed Dies of Flu and Sepsis 4 Weeks Following Work Mandated Flu Jab
A previously healthy 26 year old radiologist who was required to get a flu shot as part of her employment got flu 4 weeks after her injection and within days had developed sepsis.
Sepsis is a very serious whole-body infection brought about by illnesses, vaccinations, surgery and childbirth. It can take time to develop after the initial illness or procedure, but once it takes hold it can kill rapidly.
Cosmopolitan reported:
‘Katie McQuestion was seemingly healthy just one week before she passed away from the flu. The 26-year-old newlywed felt symptoms of influenza December 29, but things quickly worsened. On January 1, she was rushed to the emergency room with a low temperature, high blood pressure, and a high heart rate.
Twelve hours after her hospital admission, doctors told her family it was too late; she had been experiencing sepsis, a life-threatening condition, and her organs were failing. She died January 2, just months after getting married and starting a new chapter of her life.
Kenosha News reports McQuestion had the flu when she died, which led to sepsis and a heart attack. She had gotten a flu shot just a month earlier as a requirement for her job as a radiology technician and was in perfect health.
Source: Cosmopolitan, 15 January 2015.
Vaccinated Radiologist Dies of Flu and Sepsis
Despite the fact that the young woman was vaccinated and the flu and sepsis could have been triggered by the vaccine, the CDC are using her death to encourage people to get vaccinated
Girl, five, dies from a strain of the flu she was vaccinated against as deadly epidemic continues to sweep across the US
A five-year-old girl has died in hospital three days after developing a strain of the flu that she was vaccinated against – as a deadly outbreak of the virus continues to sweep across the country.
Keira Driscoll was prescribed steroids and a nebulizer at a Quick Care clinic after she started feeling unwell with a cough and a fever at her home in Clark County, Las Vegas, last Sunday.
But just hours later, she collapsed. Her mother, Tiffany Driscoll, frantically performed CPR on her small body, before she was rushed to hospital. There, she was found to have influenza A.
Despite medics’ best efforts, Keira could not be resuscitated and she was placed on life support. On Tuesday, her parents made the heartbreaking decision to turn off the machine the next day.
However, Keira died before the machine would have been switched off after suffering from a cardiac arrest. She was surrounded by her mother, father, Peter Driscoll, and other relatives at the time.
The youngster is the fourth child in the Nevada-based county – and the 56th nationwide – to have died from the flu in the past few months as vaccines have proved largely ineffective.
Is flu vaccine failure to blame for sharp rise in West Yorkshire winter deaths?
A failed flu vaccine is thought to be responsible for a sharp rise in winter deaths in West Yorkshire.
There were 1,490 excess winter deaths in the county during the winter of 2014/15, according to government figures.
This was a shocking 86% increase on the previous year.
And while winter deaths in 2015/16 declined on the previous year, it was still an increase of almost 40% than the number recorded in 2013/14, according to provisional data.
Excess winter deaths are defined as the difference between the number of deaths in the winter months (December to March) compared with the previous (August to November) and following (April to July) three months.
The total number of excess winter deaths across the UK as a whole during 2014/15 was 43,850, the highest level seen in over 15 years.
The sharp increase has been largely attributed to the failure of the flu vaccine which experts say was only effective in one in three cases.
A key contributing factor in these deaths is the high number of people in the UK still living in cold homes within rural parts of the country.
Malcolm Farrow from OFTEC, the oil heating trade body, said: “The shocking increase in the number of excess winter deaths seen over the past two years shows there is still much more that needs to be done.”
Source: The Huddersfield Daily Examiner, 29th December 2016.
VAN UK’s Comment: While they blame this on vaccine failure, repeated flu vaccines make them less effective and can even make you more likely to get H1N1. ailure, studies have shown that prior H1N1 vaccination weakens the immune response to flu.
http://www.examiner.co.uk/news/west-yorkshire-news/flu-vaccine-failure-blame-sharp-12381199
https://www.statnews.com/2015/11/11/flu-shots-reduce-effectiveness/
Study finds flu shot really did make people sicker
Calgary is Alberta’s flu hotspot, despite higher vaccination rate
Despite boasting healthy vaccination numbers, the Calgary area has been hit with 70 per cent of Alberta’s confirmed influenza cases.
Of 756 confirmed cases of influenza A, the Calgary zone’s share was 532, according to figures released Thursday by the health superboard.
And the zone accounted for 134 of 189 flu hospitalizations so far in Alberta, said the AHS.
At the same time, those who’ve received flu vaccinations in the Calgary area numbered 422,167, compared to 314,815 in the Edmonton zone, which recorded only a 10th as many influenza A cases as Calgary.
The province has also now recorded two flu-related deaths, one in the Calgary zone and the other in the southern zone.
The dramatically higher numbers in Calgary are difficult to explain, said Dr. Judy MacDonald, medical officer of health for the AHS in the Calgary zone.
“It’s a bit unusual we’ve got so much flu here and not so much elsewhere,” she said. “It started here and the other zones haven’t caught up. Maybe they will at some point.”
Source: Calgary Herald, 16th December 2016.
http://calgaryherald.com/news/local-news/despite-higher-vaccination-numbers-calgary-has-wide-lead-in-flu-cases
Getting flu shots too early raises influenza risk, say WA GPs
PHARMACIES are exposing people to the deadly flu virus during the peak of the season by encouraging customers to get their vaccination too early.
The push by chemists to “book a flu shot today” contradicts advice from the Department of Health, the Federal Government’s immunisation advisory body, the Royal Australian College of GPs and Australian Medical Association.
Official advice is that people get their flu jabs in May or early June to ensure they have the highest level of protection during the peak of the season between July and September.
Australian Technical Advisory Group on Immunisation advice states that protection against the flu starts to decrease three to four months after vaccination.
But pharmacies, including well-known chains, are encouraging early flu shots via in-store promotions, direct approaches to customers and online adverts.
Promotional materials spruik the need to get a flu shot “today” while making references to last year’s deadly influenza outbreak in the Eastern States.
Doctors slammed the pharmacy industry’s campaign as “confusing” and putting people’s health at “serious risk”.
The latest advice from Australian Technical Advisory Group on Immunisation (ATAGI) for the flu vaccine states: “recent evidence suggests protection against influenza may start to decrease from three to four months following vaccination and early vaccination needs to be balanced with this”.
RACGP president Dr Bastian Seidel said “urging patients to receive their flu vaccination too early in the year may put them at serious risk”.
“The last thing we want to see this year is patients doing the right thing and receiving a flu vaccination, only for the vaccination to wear off by the time we reach flu season,” Dr Seidel said.
AMA WA president Dr Omar Khorshid said pharmacies “are obviously motivated to get people through the door”.
“But we don’t see large numbers of people with the flu until after June … so, yes, what the pharmacies are doing has the potential to confuse many people,” he said.
Pharmacy Guild of Australia WA president Matthew Tweedie said there had already been more than 700 cases of influenza in WA this year.
This is double the number at the same time last year.
Mr Tweedie said there were benefits in getting the flu shot, regardless of the timing.
Department of Health communicable disease control director Dr Paul Armstrong said WA’s flu season typically started in June and peaked between July and September.
“DoH would recommend vaccination in May or early June, recognising the vaccine will take about two weeks before full protection is achieved,” Dr Armstrong said.
“DoH supports the RACGP’s position that it’s more important to get the timing of vaccination right, than simply to vaccinate as early as possible”.
Dr Armstrong said possible exceptions would be people living in northern Australia, including the Kimberley, where influenza started early, as well as pregnant women who should be vaccinatedat least two weeks before delivery.
He said people could seek advice from their health provider “as to the optimal timing”.
Meanwhile, the DoH revealed it would trial a mandatory “opt out” flu vaccination program for WA health workers.
Staff would be encouraged to get vaccinated or “actively decline vaccination” by stating their reasons for opting out.
Only 50.3 per cent of WA’s doctors, nurses and other healthcare workers were vaccinated last year. Dr Armstrong said although this rate had improved, it “needs to improve even further”.
University of Notre Dame’s School of Medicine dean Professor Gervase Chaney said there was “a good argument from an ethical point of view to consider mandatory vaccination”.
“I’m certainly sympathetic to the argument that the rights of the patient outweigh the rights of the individual,” he said.
Official figures showed last year’s influenza outbreak killed 546 people nationwide, mostly in the eastern states, including several young children.
There were more than 170,000 flu cases in 2017, with WA recording about 3700.
RACGP claimed the flu contributed to an average of 3000 deaths a year, 18,000 hospital admissions, while 350,000 Australians were affected by the flu.
Source: Perth Now, 24 March 2018. https://www.perthnow.com.au/news/health/getting-flu-shots-too-early-raises-influenza-risk-say-wa-gps-ng-b88784603z
Healthy, vaccinated 40-year-old among six new flu deaths in San Diego
The county Health and Human Services Agency reported six more flu-related deaths in its weekly influenza report. Among them is a 40-year-old woman from East County who died on March 14. According to county records, she was vaccinated and had no other underlying health conditions.
That specific set of circumstances, vaccinated with no other known health problems, has been very rare among flu-related deaths this year.
Source: The San Diego Union Tribune, 21 March 2018. http://www.sandiegouniontribune.com/news/health/sd-no-flu-update20180321-story.html |